
The lower end of the esophagus does not open up(relax) when food comes in, resulting in a block in the lower end of the food pipe(food stuck there).The motility (propulsion of food) in the body of the esophagus is also not there. So, food starts getting accumulated in the food pipe, causing it to dilate over time.
Patients with achalasia experience symptoms that gradually worsen over time.
Typical symptoms include:
Achalasia affects both men and women equally, most commonly between the ages of 20 and 50 years. It is rare in children, accounting for only 2–5% of cases.
Achalasia occurs due to damage or loss of nerve cells (ganglia) in the lower esophagus and the lower esophageal sphincter (LES).
These lead to the sphincter remaining tightly closed and the esophagus losing its ability to push food downward.
Diagnosis involves a stepwise approach to confirm the condition and rule out other causes of blockage.

The main goal of treatment is to relieve swallowing difficulty, prevent food stagnation, and reduce complications.


Removal of the entire esophagus in advanced, long-standing cases (sigmoid or megaesophagus).
Medicines are usually prescribed when patients are not fit for or refuse surgical/endoscopic therapy.
Untreated achalasia can lead to:
Current treatments relieve symptoms effectively, but restoring normal peristaltic movement of the esophagus is uncommon.
Recovery depends on the chosen treatment:
Each treatment carries specific risks:
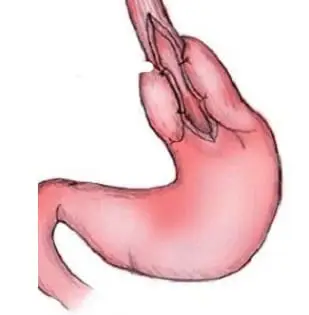
It is a minimally invasive surgical procedure done through 3–4 small holes using laparoscopy. The non-relaxing muscles at the lower end of the food pipe (esophagus) are cut to relieve the blockage. A partial fundoplication (wrapping part of the stomach around the lower esophagus) is added to prevent food and acid from refluxing back into the esophagus.
The hospital stay is usually 2–3 days.
Yes. It is a major surgery performed under general anesthesia. It is a technically demanding procedure that should be done by experienced gastrointestinal surgeons.
Symptom relief is usually dramatic. Difficulty in swallowing improves significantly, patients can eat normally, regain lost weight, and become healthy again. Heartburn, cough, and wheezing caused by reflux also get completely relieved after surgery.
Symptom relief is almost immediate.
On the day after surgery, a dye test (contrast swallow study) is done to confirm that the blockage is relieved. Patients usually feel the improvement right away.
Laparoscopic Heller’s Cardiomyotomy is considered the gold standard treatment for achalasia cardia. It not only relieves the blockage but also helps prevent reflux due to the added fundoplication.
In contrast, POEM (Peroral Endoscopic Myotomy) carries a higher risk of perforation (hole) in the esophagus, which can be life-threatening, and has a 100% chance of reflux after the procedure.
Our expert team provides world-class treatment for Achalasia Cardia and other gastrointestinal diseases using advanced techniques and compassionate care. We focus on restoring your ability to swallow and improving your quality of life.
📞 Book your appointment today to consult our specialist gastro for timely diagnosis and treatment of Achalasia Cardia.